


Personalized nutrition is somewhat of a buzzphrase in the health and wellness world, appearing everywhere from women’s magazine covers promising that your DNA can assist you in losing weight to scientific journals comparing omics (study of the proteome, metabolome, genome, etc.) to optimal eating patterns.
With the world facing a pandemic of obesity and chronic disease, the desire to revamp the modern diet is understandable. Personalized nutrition aims to solve this issue by gathering individual data to develop targeted nutritional advice or products.
As with most emerging fields of study, personalized nutrition is often framed with false or questionable beliefs. This post hopes to shine a light on some of them.
- Myth 1: It’s expensive to get a personalized nutrition plan.
- Myth 2: Personalized nutrition is a fad weight loss diet.
- Myth 3: Men and women should eat the same.
- Myth 4: Food intolerances are not more common nowadays; we are just more aware.
- Myth 5: DNA is the most important predictor of our unique nutrition blueprint.
- Myth 6: Personalized nutrition diets are restrictive.
- Myth 7: Personalized nutrition is an oversaturated market.
- Conclusion
Myth 1: It’s expensive to get a personalized nutrition plan.
False!
The term “personalized nutrition” started gaining traction when scientists first succeeded in sequencing the human genome in 1990.[1] This raw data at the intersection of medicine and bioinformatics promised the imminent arrival of personalized medicine and nutrition.
Because of the history, individual genotyping – a typically expensive process – is still most often referred to in personalized nutrition. However, simple diagnostic tools to assess the physical and metabolic profile of an individual are now becoming more important and relevant. This variety of tools ranges from simple questionnaires to widely used inexpensive wearables (such as a continuous glucose monitor) and food sensitivity tests to finger prick or gut microbiome tests.
Nutrition can be personalized based on genotypic information (the genes and their expression) or phenotypic information (e.g., age, BMI, sex, and biological responses to food).
Companies offering personalized nutrition nowadays usually leverage artificial intelligence and machine learning approaches to integrate all this data into a life-improving personalized diet plan.
Myth 2: Personalized nutrition is a fad weight loss diet.
False!
Fad diets promise quick weight loss, which can come at the cost of nutritional deficiencies, negatively impacted hormonal health and metabolism, and stress and anxiety over food choices.
The premise of personalized nutrition is different. It offers a long-term change in eating habits that results in better physical and mental health, improved gut health and digestion, more energy, and an overall more optimized way of living.
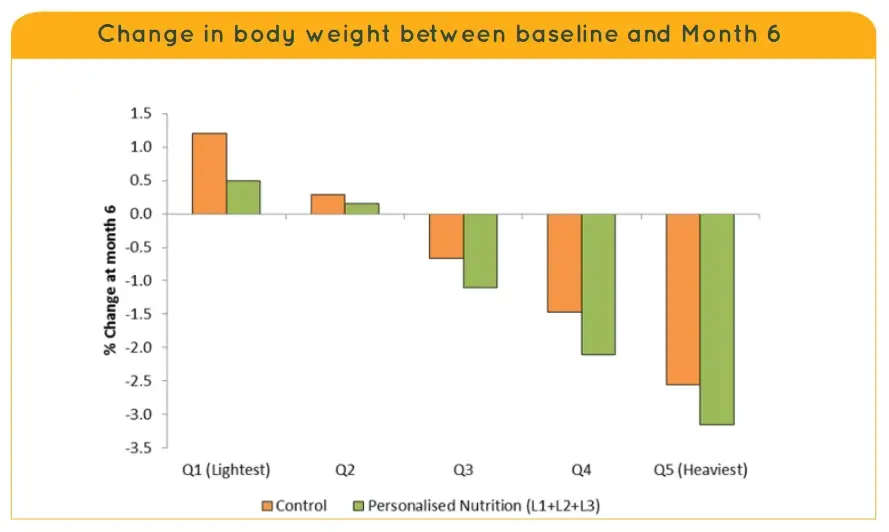
A 2015 personalized nutrition study[2] has shown that individuals will lose weight if they are overweight and gain weight if they are underweight. That means that rather than strictly promote weight loss, personalized nutrition plans usually lead the individuals to their “body weight set point,” the natural weight that the body craves to be at to optimally perform vital functions.[3]
Myth 3: Men and women should eat the same.
False!
Sex plays a significant role in personalized nutrition. Women process nutrients differently than men and need specific nutrients at each life stage as well as each part of the cycle.
For example, the transport of fat in the bloodstream is almost twice as fast in women as in men, which can significantly increase the risk of cardiovascular disease.[4] Men and women also respond significantly differently to anti-inflammatory nutritional interventions.[5] And with obesity set to overtake smoking as the largest preventable cause of cancer in women[6], it is important to embrace these differences to promote individual health.
Until around 1990, dietary guidelines were based solely on research in men (for Americans, the subjects of the research were men enlisted in the military). Even after women’s health appeared on the radar, it was mostly addressed in the realm of reproductive health. Today, more and more nutrition studies look at men and women separately for how certain nutrients affect certain processes.
Myth 4: Food intolerances are not more common nowadays; we are just more aware.
False!
Food intolerance or food sensitivity tests are very often a part of crafting a personalized nutrition plan. They can be performed at a doctor’s office or at home with a cheek swab, saliva swab, or finger prick.
And while some skeptics downplay food sensitivities as personal choices or fussiness, it is an irrefutable fact that food allergies and intolerances are on the rise in the US and other industrialized countries around the world.[7] At this moment, around 6 million American children have an identified food allergy. That is two kids in every classroom.[8]
It is important to note that a food allergy is not the same as a food sensitivity. A reaction to an allergy is triggered by the immune system, while a reaction to sensitivity occurs in the digestive system. Unlike an allergy, sensitivity or intolerance is not life-threatening. Still, its symptoms ranging from bloating to skin rashes, can undoubtedly hinder the quality of life, which is why it’s essential to consider both when creating a personalized nutrition plan.
Myth 5: DNA is the most important predictor of our unique nutrition blueprint.
False!
An “old-school,” purely genome-based personalized nutrition plan would indicate that identical twins who share the same DNA would have the exact same dietary needs. But the human body is such a complex system that even identical twins can have significantly different responses to food Some factors that influence these different responses are:
- the way the body digests and breaks down carbohydrates and fats from food
- how much and for how long blood fat and blood sugar levels rise and fall after eating
- the composition of the gut microbiome
- the number and sequence of meals
- the quality of sleep
- the amount and level of exercise
Myth 6: Personalized nutrition diets are restrictive.
False!
Rather than focusing on a single indicator of health (usually weight), personalized nutrition is a pursuit of overall better health. This includes physical health, which means optimal body weight, more energy, stamina, better sleep, etc. It also includes mental health, social health, emotional wellbeing, and even one’s financial health. A personalized nutrition plan can adapt to one’s biological needs just as much as it can adapt to the availability of food in their area, their budget, the number of people they might be cooking for, and so on.
A personalized diet also doesn’t promise any quick results. Instead, it encourages mild, commonly accepted dietary guidelines, such as drinking plenty of water, eating whole foods that fit the individual’s profile, and incorporating movement into everyday life.
Restriction, often encouraged by standard healthy diets, can quickly lead to loss of motivation, physical and mental weakness, lowered metabolic function, lowered immunity, and may even lead to eating disorders. Personalized nutrition, on the other hand, empowers the individual to eat and live in a way that gives them more energy, satisfaction, and a higher quality of life.
Myth 7: Personalized nutrition is an oversaturated market.
False!
While more and more companies understand the appeal of this field, there are still many unoccupied spaces in this market territory that is set to grow more than three-fold by 2030.[9] The recent pandemic has shifted customers’ perspective more toward care for their own health, well-being, and immunity. This shift drives a growing market need for a plethora of personalized nutrition products and services – from coaching to dietary supplements and functional foods.
Conclusion
Personalized nutrition suggests nutrition advice tailored to an individual’s specific needs rather than repeating broad, one-size-fits-all guidelines.
Foods affect everyone differently, and the response to foods is highly related to the risk of long-term diseases. Personalized nutrition plans are also more likely to improve the quality of life than general health advice, according to large-scale studies.
Suggestic has been at the forefront of this issue since 2014, enabling health organizations to build and deliver personalized nutrition programs at a fraction of time and cost. Rather than taking a singular approach to personalization (such as DNA only), our multifaceted software will consider every single piece of data you feed it: from simple phenotypic information (such as sex, age, and BMI), food restrictions, availability, and preferences, to real-time data from user devices and all kinds of clinical lab results.[10]
To get a taste of Suggestic’s hyper-personalization abilities, check out how you can use our platform to create meal plans or nutrition programs for your clients.
References
| 1 | Pillsbury, E. (n.d.). Genome Sequencing: A History. [online] Yale University. Available at: http://bioinfo.mbb.yale.edu/course/projects/final-4/ |
|---|---|
| 2 | Gibney, M., Walsh, M. and Goosens, J. (n.d.). Personalized Nutrition: Paving the way to better population health. [online] Available at: https://www.karger.com/Article/Pdf/452389 |
| 3 | Dieter, B. (n.d.). Understanding Set Point Theory in a Nutrition and Weight Loss Context. [online] blog.nasm.org. Available at: https://blog.nasm.org/set-point-theory [Accessed 27 Oct. 2022] |
| 4 | Nutrition Insight. (n.d.). Sex matters: Gender-specific science advances as demand for tailored nutrition surges. [online] Available at: https://www.nutritioninsight.com/news/sex-matters-gender-specific-science-advances-as-demand-for-tailored-nutrition-surges.html [Accessed 27 Oct. 2022] |
| 5 | McMorrow, A.M. et al. (2018). Personalized Cardio-Metabolic Responses to an Anti-Inflammatory Nutrition Intervention in Obese Adolescents: A Randomized Controlled Crossover Trial. Molecular Nutrition & Food Research, 62(10), p.1701008. doi:10.1002/mnfr.201701008 |
| 6 | Cancer Research UK (2018). Obesity could overtake smoking as biggest preventable cause of cancer in women. [online] Cancer Research UK – Cancer News. Available at: https://news.cancerresearchuk.org/2018/09/24/obesity-could-overtake-smoking-as-biggest-preventable-cause-of-cancer-in-women/ [Accessed 27 Oct. 2022] |
| 7 | Prescott, S.L. (2013). A global survey of changing patterns of food allergy burden in children. World Allergy Organization Journal, 6(1), pp.1–12. doi:10.1186/1939-4551-6-21 |
| 8 | Gupta, R.S. (2019). Prevalence and Severity of Food Allergies Among US Adults. JAMA Network Open, [online] 2(1), p.e185630. doi:10.1001/jamanetworkopen.2018.5630 |
| 9 | Precedence Research (n.d.). Personalized Nutrition Market Size, Share, Report 2022-2030. [online] www.precedenceresearch.com. Available at: https://www.precedenceresearch.com/personalized-nutrition-market [Accessed 27 Oct. 2022] |
| 10 | Jinnette, R. (2020). Does Personalized Nutrition Advice Improve Dietary Intake in Healthy Adults? A Systematic Review of Randomized Controlled Trials. Advances in Nutrition. doi:10.1093/advances/nmaa144 |